
Boost Teamwork: Healthcare Team Communication Guide
Get our practical guide to healthcare team communication. Fix broken workflows, reduce errors, & build cohesive teams in 2026.
Dan Robin

A nurse spots a lab result that doesn't fit the patient's trend. She pages the physician, then sends a secure message, then asks the charge nurse if anyone's seen him. By the time the loop closes, the patient has changed and everyone involved feels like they did their part, even though the system clearly didn't.
The Communication Breakdown We All Pretend Is Normal
If you spend enough time in hospitals, you stop being surprised by broken communication. That's the problem. We start treating it like weather instead of a fixable operating issue.
A missed callback. An order that was discussed but never entered. A handoff that technically happened, but left out the one detail that mattered. None of this looks dramatic in isolation. On the floor, it just feels like friction. A little delay here. A little guesswork there. But stack enough of those moments together and you get a care environment where people spend half their energy chasing clarity.
Small misses become system failures
This isn't about bad people doing careless work. It's about expecting clean coordination inside a messy system. A patient may interact with about 50 different employees during a 4-day hospital stay, and observational research found about 30% of team interactions during surgery involved a communication failure, according to NIH's summary of team communication research. When that many people touch the same patient, handoffs stop being administrative details. They become the work.
I've seen administrators look at this and say, “We need people to communicate better.” That sounds reasonable. It's also incomplete. People can be thoughtful, skilled, and well-intentioned, and still fail inside a process that relies on memory, hallway updates, and whichever device someone happens to check first.
Practical rule: If critical information depends on one person remembering to chase another person, you do not have a communication process. You have a hope-based workflow.
We confuse effort with reliability
Healthcare teams are full of people making heroic workarounds. Nurses act as go-betweens. Unit clerks patch holes. Residents carry details in their heads because the handoff note is thin. Charge nurses become air traffic control.
That improvisation keeps care moving. It also hides the size of the problem. Leaders see that the unit “got through it” and conclude the current setup is acceptable. It isn't. It's expensive in attention, morale, and safety.
If you want a useful mental model, it helps to go back to the benefits of interpersonal communication. The basics still matter. Clear listening, confirmation, context, trust. But in hospitals, those basics have to survive noise, hierarchy, shift changes, and time pressure. That's why goodwill alone won't save you.
Normal doesn't mean acceptable
A lot of what passes for normal in hospital communication would be unacceptable in any other high-risk operation. People wait on unread messages. Teams use separate tools that don't talk to each other. Vital context gets buried in free text or verbal updates.
Staff adapt because they have to. Patients pay the price when adaptation isn't enough.
The first step is simple and uncomfortable. Stop calling these issues “soft.” They're operational failures wearing human faces.
Why Poor Communication Is a Clinical Risk
For years, communication got shoved into the same bucket as bedside manner, meeting etiquette, and leadership style. Nice to have. Good for culture. Helpful if you can get to it.
That framing has done real damage. Communication in healthcare is a safety function.
Early in any improvement effort, I tell leaders to stop asking whether communication training is worth the time. Ask what unmanaged communication failure is already costing you in risk, rework, and avoidable harm. That usually changes the conversation fast.

The numbers are blunt
The Joint Commission has reported that 80% of serious medical errors were caused by miscommunication between caregivers, and patients receiving care from poor teams were almost five times as likely to experience complications or death, based on evidence summarized by HIPAA Journal's review of poor communication in healthcare. That is not a side issue. That is a core clinical risk.
What matters here isn't just the severity. It's the pattern. Communication failures don't only show up in rare disasters. They sit inside ordinary care. Consults, discharges, escalations, transfers, medication clarifications, post-op updates. The places where work moves from one person to another are where harm gets invited in.
Soft skill is the wrong label
When people hear “communication,” they often think personality. Is someone polished? Direct? Likable? That's not the question. The critical question is whether the team can move accurate, time-sensitive information from the right person to the right person fast enough to support safe decisions.
A hand hygiene protocol is a safety system. A surgical timeout is a safety system. Standardized communication belongs in the same category.
Poor communication doesn't stay poor communication for long. It turns into delay, duplication, confusion, and eventually patient harm.
Clinical competence includes information transfer
Some leaders still separate technical excellence from communication quality, as if one is clinical and the other is cultural. On the floor, that distinction falls apart. A perfect clinical judgment that never reaches the right person in time is operationally useless.
Three practical implications follow from that.
Standardization matters: Teams need a shared way to escalate concerns and hand off care, especially when the day is busy.
Confirmation matters: Sending information isn't enough. The receiver has to understand it, and the sender has to know that happened.
Visibility matters: If key updates live in too many places, staff will miss them, even when they're trying not to.
Once you accept that communication is part of clinical competence, a lot of fuzzy debates disappear. You stop arguing about whether to invest in it. You start asking where the handoff is weak, where escalation stalls, and which routines need structure.
The Daily Hurdles to Clear Communication
The reason healthcare team communication breaks down isn't mysterious. The work environment is built for interruption.
Shift change starts and everyone is trying to compress a complicated patient story into a few rushed minutes. In the ED, the physician is answering one question, the nurse is handling another, and both are getting pinged by different tools. On inpatient units, the same update might travel by pager, phone, secure chat, and a note in the record, with nobody fully sure which channel counts as the definitive one.
Handoffs are where the cracks widen
A bad handoff rarely looks bad in the moment. It looks efficient. Quick summary. A few shorthand phrases. Maybe a “call me if anything changes.” Then the receiving clinician inherits uncertainty and has to reconstruct the story while the shift is already moving.
What gets lost is often the part that doesn't fit neatly into a checkbox. Why the team was worried overnight. Which family concern changed the plan. Which symptom looked minor at first but kept nagging at the bedside.
That's why communication problems often feel invisible to leadership. They don't always create obvious events right away. They create ambiguity. And ambiguity makes people slower, less confident, and more dependent on workarounds.
Too many tools create false confidence
Hospitals often respond to communication friction by adding another channel. A better pager. A secure messaging app. A call system. A voice device. An EHR alert. Each tool solves one problem and creates two more if it isn't tied to the actual workflow.
I'd rather see a team use fewer channels with clear rules than stack shiny tools on top of confusion. If you're sorting through options, this guide to workforce management software for healthcare is useful because it forces the practical question leaders often avoid. Does the tool fit the way staff work across shifts, units, and roles?
The best communication tool is not the one with the most features. It's the one staff can trust under pressure.
Hierarchy and noise still get in the way
Technology isn't the only barrier. A new nurse may hesitate to escalate to a physician who's known for brushing people off. A tech may notice something concerning and still stay quiet because the unit culture says that observation belongs to someone “higher up.” Support staff may know exactly where the process is breaking and have no clean way to say so.
Then add the physical environment. Alarms. Phones. Side conversations. PPE. Doorways. Distance. Competing priorities. Healthcare is full of settings where the signal has to fight the noise.
That's why fixes based on “please communicate better” almost always disappoint. The friction is built into the day. You have to design around it.
Simple Frameworks for Complex Conversations
When the environment is noisy, structure helps. Not because people become robots. Because stressed humans need a shared script in critical situations.
That's where frameworks like SBAR and I-PASS earn their keep. They don't make conversations formal for the sake of formality. They reduce the odds that a key detail gets buried under urgency, hierarchy, or habit. And because communication failures contribute to 60% of adverse events in hospitals, standardized tools like SBAR should be treated as an error-control mechanism, as explained in Dialog Health's overview of communication between healthcare professionals.
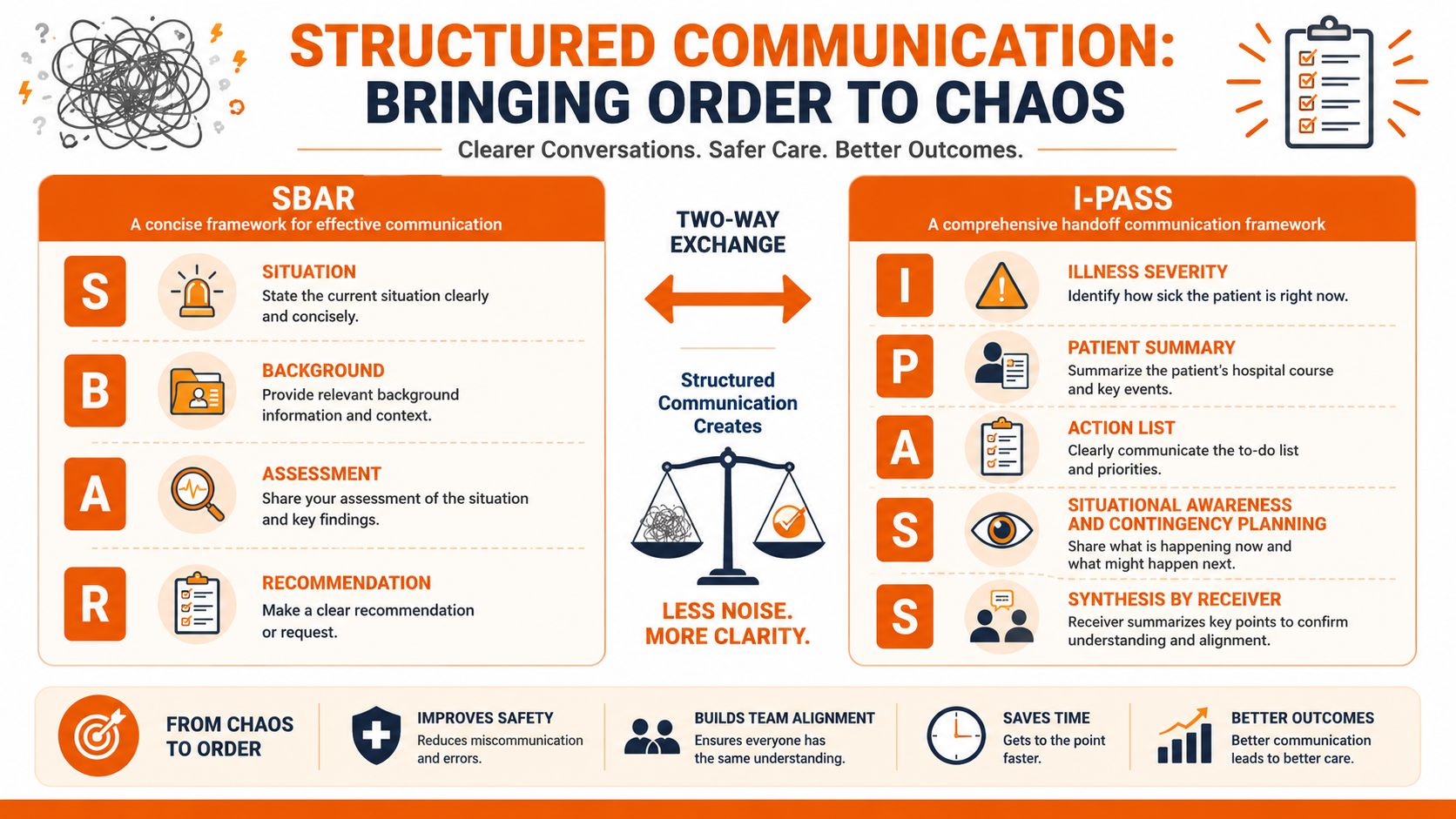
SBAR works because it respects time
SBAR stands for Situation, Background, Assessment, Recommendation. The beauty of it is that it matches how busy clinicians think when they need to act.
A nurse calling a physician doesn't need to narrate the whole shift from memory. SBAR gives the update a spine.
Situation: What's happening right now.
Background: What the receiver needs to know to make sense of it.
Assessment: What you think is going on.
Recommendation: What you need or suggest next.
Used well, SBAR cuts through rambling updates and timid escalation. It gives the sender permission to state concern clearly. It gives the receiver a cleaner path to decision-making.
I-PASS is built for handoffs
I-PASS is especially useful when care is moving between clinicians, such as end-of-shift or service transitions. It pushes teams to include illness severity, a clear patient summary, an action list, situational awareness with contingency planning, and a synthesis by the receiver.
That last part matters more than many teams realize. The receiver doesn't just nod and move on. They restate the plan in their own words. That simple habit catches misunderstandings before they become overnight surprises.
One habit worth enforcing: The handoff is not complete until the receiving person shows they understood the plan.
Communication frameworks at a glance
Framework | Primary Use Case | Key Strength |
|---|---|---|
SBAR | Urgent updates, escalation, calling a provider | Fast, concise structure for high-pressure conversations |
I-PASS | Shift changes, service transfers, resident sign-out | More complete handoffs with explicit action lists and receiver synthesis |
Don't turn the framework into theater
Organizations frequently misstep. They train the acronym, put it on a poster, and assume the job is done. Six months later staff can recite the letters but still default to uneven handoffs because the workflow never changed.
A framework only works if the team agrees on where it will be used, what “good” sounds like, and how people will practice it. Keep it narrow at first. One unit. One handoff point. One escalation process.
If you make it too broad too soon, it turns into compliance theater. Staff will say the words and skip the discipline.
A Practical Plan for Better Team Communication
Most communication improvement efforts fail for a boring reason. They try to fix everything at once.
A better approach is smaller and less glamorous. Pick one breakdown that staff complain about without needing to be prompted. Night-to-day handoff on one unit. Escalation to the on-call physician. Discharge coordination between case management and nursing. Start where the pain is obvious and repeated.

Start with one workflow, not a grand campaign
Walk the process as it really happens. Not the policy version. The actual version. Ask frontline staff where they lose time, where they repeat themselves, and where they don't trust the handoff.
Then tighten one thing.
Define the trigger. Be specific. “Any change in patient condition” is too vague. “Escalation after concerning lab result” is concrete.
Choose the communication path. Decide which channel is primary and which one is backup. If staff have to guess, they will split across tools.
Add a shared format. SBAR or a handoff template serves as a shared format.
Make confirmation visible. The sender needs to know the message was received and understood.
That alone fixes more than another policy memo ever will.
Build feedback into the system
Leaders often focus on downward communication and forget the harder part. Staff need a safe, regular way to tell you what isn't working. Public guidance highlighted by Tulane's public health review notes that the CDC and AHA recommend regular feedback loops, anonymous input channels, and visible follow-through as part of stronger healthcare communication systems, which you can read in this discussion of communication in healthcare.
Visible follow-through is the piece most organizations miss. If staff raise the same issue three times and nothing changes, they stop reporting. Then leaders think silence means stability.
A simple operating rhythm works better than a big annual initiative:
Weekly check-ins: Ask one focused question about communication friction.
Anonymous reporting option: Some staff will only tell the truth if their name isn't attached.
Closed-loop updates: Tell people what changed, what didn't, and why.
Use tools that reduce fragmentation
The right tool should reduce channel sprawl, not add to it. In practice, I look for a few things. Role-based communication. Mobile access for staff who aren't at desks. Team spaces for unit-level coordination. A searchable place for policies and updates so people don't go hunting across inboxes and shared drives.
One option in that category is communication software for healthcare companies, including platforms like Pebb that combine team chat, updates, calls, files, and operational information in one place. That doesn't remove the need for process design. It just gives the process a cleaner home.
Don't confuse morale events with communication systems, either. Team bonding has value, and some leaders get ideas from resources like top corporate team building ideas. But no offsite, lunch, or escape room will fix a handoff process that depends on three apps and a prayer.
Roll out gently
You do not need a hospital-wide launch on day one. Pilot with a team that feels the problem and wants relief. Watch what they do. Adjust. Then expand.
The point isn't perfection. It's reliability people can feel in a real shift.
How to Know if Your Communication Is Improving
A lot of teams measure communication the lazy way. They count messages, app logins, or training completion and call it progress.
Those numbers might tell you whether a tool is being touched. They won't tell you whether healthcare team communication is getting safer, clearer, or less frustrating.
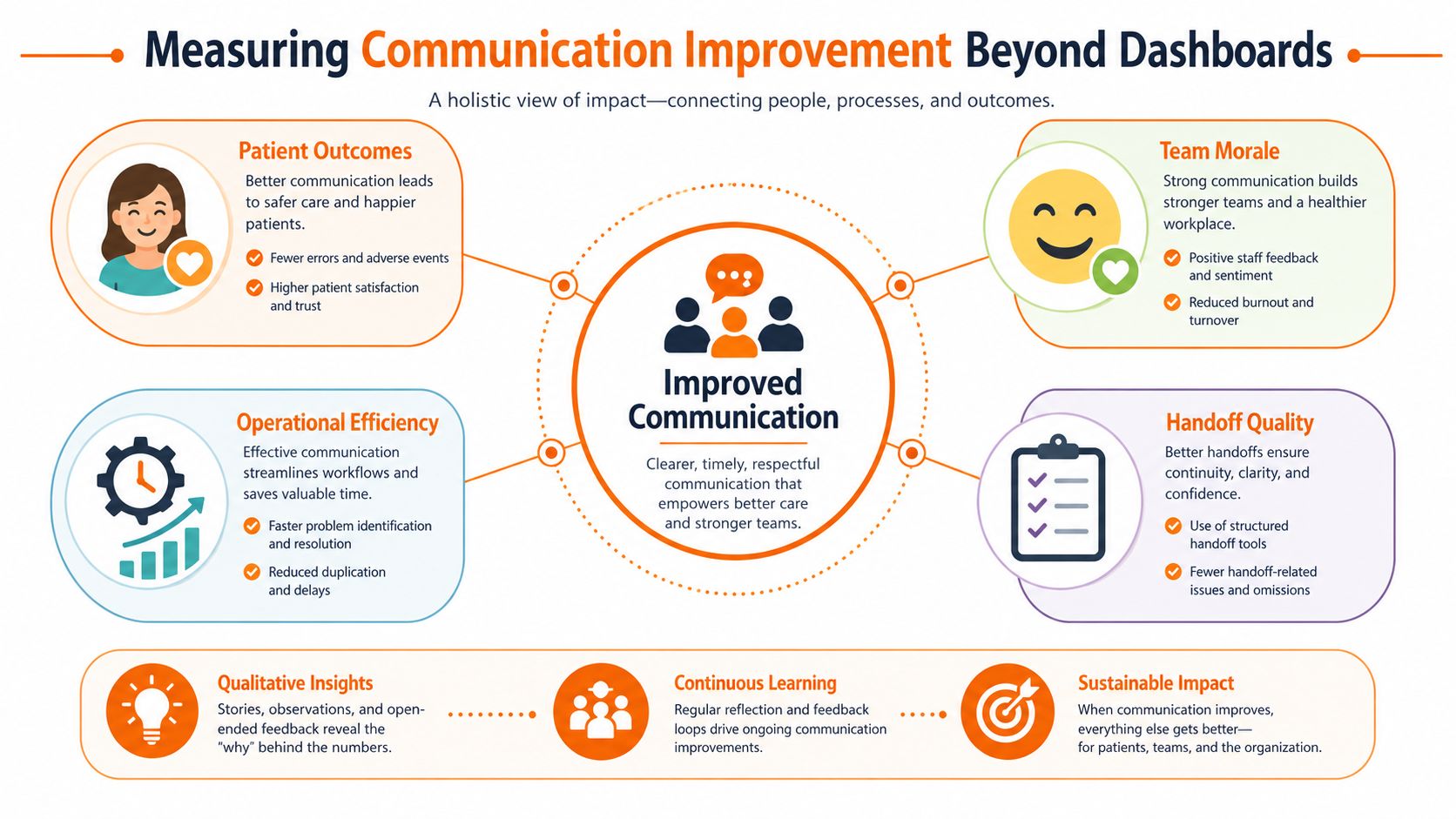
Look for operational proof
The best signs of improvement show up in the work itself. Staff stop chasing missing information. Escalations happen earlier. Handoffs become more consistent from one clinician to the next. Fewer people say, “I didn't know that,” or “I thought someone else called.”
You don't need a fancy dashboard to start seeing this. You need disciplined observation.
A practical review should look at four lenses:
Handoff quality: Sample handoffs and listen for missing context, unclear action items, and weak receiver confirmation.
Team friction: Ask staff where communication still breaks down during a normal shift.
Response reliability: Check whether urgent requests consistently reach the right role without extra chasing.
Incident themes: Review reports for recurring communication patterns, not just isolated mistakes.
Mix staff feedback with workflow evidence
Leaders sometimes trust only hard metrics, then miss the early warning signs that frontline teams can feel before they can quantify them. Other leaders rely only on anecdotes, which can drift into opinion and politics.
You need both. Staff feedback tells you where the process still feels brittle. Workflow review tells you whether those concerns show up in the actual mechanics of care. If both point to the same weak spot, you've found the next problem to solve.
This article on how to measure communication effectiveness is useful because it pushes beyond vanity measures and toward signs that the system is healthier.
If your only evidence of improvement is that more messages were sent, you probably improved activity, not communication.
Watch for signs of trust
The strongest communication systems have one quality that doesn't fit neatly in a spreadsheet. People trust them.
You hear it in the way staff talk. They know which channel to use. They believe concerns will be heard. They expect handoffs to include what matters. They don't spend the first hour of every shift reconstructing missing context from scraps.
That's what you're trying to build. Not more communication. Better transfer of meaning under pressure.
The Work Is Never Really Done
Communication is not a project you finish. It's a practice you maintain.
Hospitals change constantly. New staff arrive. Units get busier. tools multiply. Workflows drift. A process that felt solid six months ago can get shaky fast if nobody is tending it. That's normal. The answer isn't another slogan about teamwork. It's steady attention to the places where information gets lost, delayed, softened, or ignored.
The good news is that this work compounds in a healthy way. One cleaner handoff can lower stress for a whole shift. One reliable escalation path can change whether a nurse speaks up next time. One feedback loop that leads to visible action can rebuild trust that's been thin for years.
That's usually how healthcare team communication gets better. Not through a grand fix. Through repeated, practical choices that make the next conversation clearer than the last.
If you're trying to bring communication, updates, tasks, files, and day-to-day coordination into one place for frontline and office staff, Pebb is worth a look. It gives teams a single app for chat, voice and video calls, news-feed style updates, team spaces, documents, and operational workflows, which is useful when you're trying to reduce fragmentation instead of adding another disconnected tool.
